

ARCHIVES
Potential Briefs
ISSUE #02 — APRIL 2011
Comment on this Newsletter... CLICK HERE
ARTICLE HIGHLIGHT
Dhiraj Jeyanandarajan, M.D. - Board Certified Neurologist
Article: Protecting the Genitofemoral Nerve during Direct/Extreme Lateral Interbody Fusion (DLIF/XLIF) Procedures
Authors: Faisal R. Jahangiri, Jonathan Sherman, Andrea Holmberg, Robert Louis, Jeff Elias, Francisco Vega-Bermudez
Journal: Am J Electroneurodiagnostic Technologists 50:321-325, 2010
Summary: This paper is a case study of a patient undergoing a direct lateral interbody fusion (DLIF) procedure with multimodality monitoring employed to protect the nervous system structures at risk. Somatosensory evoked potentials (SSEPs) of the lower extremities included posterior tibial nerve and femoral nerve stimulation to monitor the integrity of the lumbar plexus and dorsal column of the spinal cord. Upper extremity SSEPs were employed to monitor for positioning effect. Spontaneous and triggered electromyography (EMG) were utilized to check for nerve root irritation when advancing through the psoas muscle and during the procedure itself. Triggered EMG of the cremaster muscle during the approach allowed for identification of the genitofemoral nerve and subsequent redirection of the probe.
The author's conclusions are that during this DLIF procedure, multimodality monitoring including recording T-EMG of the cremaster muscle was effective at identifying proximity to the genitofemoral nerve. More generalized, they concluded that multimodality monitoring including SSEPs (posterior tibial, femoral and ulnar nerves along with MORE
PROCEDURE REVIEW
Daniel Slepian, PA CNIM
Approach: Lateral for the Interbody Fusion and Posterior for Transpedicular Fixation.
Indications: Spinal Deformity, Degenerative Disease
The lateral approach is an excellent option to treat degenerative spinal disease. After positioning the patient in the right lateral decubitus, the table is jack-knifed to permit improved access to the disc levels to be addressed, most commonly, L2-3, L3-4 and L4-5. Disc levels can be easily identified using C-arm imaging.
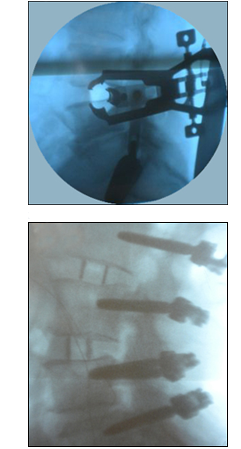
The procedure is accomplished by passing through the psoas muscle as the disc level is approached. Once accomplished, the disc is incised and removed through the retractor using disc rongures and curettes. The disc space is sequentially distracted with trial implants, eventually achieving a satisfactory disc space height. Once a specific size is selected, the graft with radiolucent markings can be impacted into the disc space and visualized with a C-arm image.
The retractor is clearly visable in the top x-ray. The x-ray below shows an anterior interbody fusion and posterior fixation.
ILLUSTRATION REVIEW
Vastus Lateralis, Tibialis Anterior, Gastrocnemius
The muscle groups illustrated below may be used to monitor lateral procedures of the lumbar spine. The transverses abdominis not illustrated but is an option to consider for the first lumbar nerve root (L1).
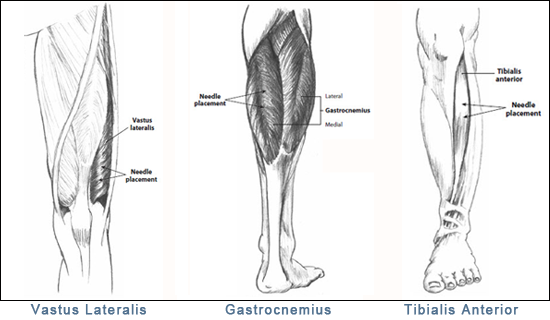
Vastus Lateralis
Action: Extends and rotates the leg, helps to maintain the patella in its groove during extension.
Innervation: Femoral nerve, L2, L3 (Primary), and L4 (primary).
Gastrocnemius
Action: Plantar flexes the foot and flexes the knee.
Innervation: Tibial nerve, S1 (primary) and S2.
Tibialis Anterior
Action: Flexes the ankle joint dorsally and inverts the foot.
Innervation: Deep peroneal nerve, L4 (primary) and L5.
This site, along with other muscles of the distal extremities, has been found to be optimal for tceMEPs. Additional muscle groups may be monitored to provide added information, but data are generally considered to be less reliable.
WEBSITE VIDEO TOUR
Richard Slepian - President