

ARCHIVES
Potential Briefs
ISSUE #03 — MAY 2011
Comment on this Newsletter... CLICK HERE
ANNOUNCEMENTS
Annual ASNM Conference
Stop by the ORIMtec booth and page through our recently released 3rd edition of the Neurotechnologist Reference Guide. See why over 800 copies have been distributed worldwide.
Have you participated in our recent poll, "Who Should be Approved to Supervise IONM Technologists"? Come by our booth or vote here!
ARTICLE HIGHLIGHT
Dhiraj Jeyanandarajan, M.D. - Board Certified Neurologist
Article: Cervical Spine Motion Generated With Manual Versus Jackson Table Turning Methods in a Caveric C1-C2 Global Instability Model
Authors: Christian DiPaola MD, Bryan Conrad MEng, MaryBeth Horodyski EdD, Mathew DiPaola MD, Andrew Sawers MD, Glenn Rechtine MD
Journal: Spine 2009 Volume 34, Number 26, pp 2912-2918
Summary: This paper is a cadaveric biomechanical study where the objective was to quantify spinal motion created through transferring and flipping patients with global C1-C2 instability. When positioning patients in the operating room from supine to prone there is a significant amount of motion generated that can have deleterious effects on preexisting spinal trauma and instability. Occipitocervical and/or atlantoaxial pathology can have particularly devastating outcomes given the level of cord injury that can occur. The authors use a cadaveric model and test the Jackson table against the traditional log roll technique used to position patients.
The Jackson technique involves sliding the supine patient onto the Jackson table with in line cervical stabilization. The patient is secured to the table and then the table frame is lowered over the patient, thereby... MOREINSTRUMENT REVIEW
Jackson OSI Table
The Jackson OSI table provides a multi-functional approach to patient positioning during spinal surgery. This table can be safely rotated 180 degrees while the patient is in a prone or supine position. Patient repositioning is accomplished in a safe and efficient manner, minimizing patient movement when unstable spinal pathology is a concern. The table permits multiple intraoperative x-ray or C-arm images of the spine to be taken during surgery.
On a cautionary note, the use of this equipment must be carefully monitored. Proper protocol includes the use of four persons to verify pin and safety belt placement: two are required to unlock the table and all four are needed to safely perform the table flip. For the IONM technologist, special care must be taken prior to the flip to ensure that cable placement is secure and unobtrusive, preferably by affixing cables and electrodes closely to the patient's body with the use of surgical tape. It is very important for the technologist to confirm with the anesthesiologist when they are ready for the rotation.
We have found this table to be an excellent tool for optimal patient positioning and access in the surgical environment.

ADVANCING the IONM PROFESSION
IONM at a Crossroad
The IONM specialty is at a crossroad. Do we continue to provide services in a fractured, independent manner as we do today or do we pay attention to the recommendations of the IONM Strategic Healthcare Summit? The IONM Healthcare Summit, sponsored by the ASNM, took place December 3rd and 4th in Chicago.
The primary finding at this conference was that if we are to survive and thrive as a specialty we must become a cohesive group including technologists, oversight professionals, surgeons, anesthesiologists, nurses and other OR personnel. We have what it takes to bring this all together including the brightest minds in their respective fields, but we must combine our efforts to maximize the value of our services to the patient, surgeon, hospital, payer and ourselves.
Two full days were devoted to four crucial areas of IONM including; technology, quality, provider and economics. To participate in the solution, review the Summit Summary created by the committee and be sure to go your committee of choice in the IOM Forum. Express your interest, concerns, and support.
CABLE MANAGEMENT
Cable Management Prior to the Jackson OSI Table Flip
 Prior to Rotating
Prior to Rotating
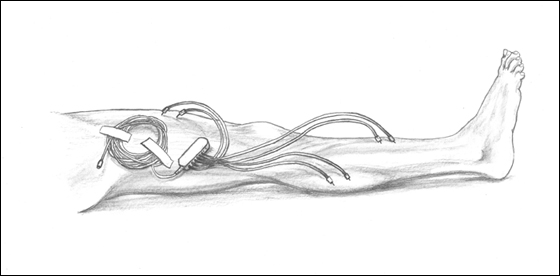
Secure the patient between the top and bottom of the OSI table. It is important to disconnect the stimulating (SSEP/DEP) and recording (EMG) cables from the amplifier. Wind them up tightly and secure them with tape to the side of the patient's leg as shown in the lateral view above.
The scalp needle electrodes should be completely removed for safety reasons. This cable can be left on the floor as long as the OSI table will continue to be used. If a different table is to be used, wind the cable up from the pod end and store it with the amplifier until it is needed again.
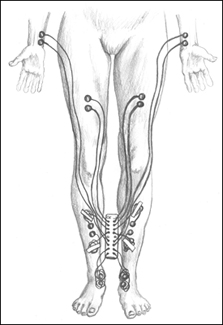
In the AP View
The stimulation box is secured between the legs and should be inverted so the input side will be face up once the patient is rotated. Remove the extension cable and store adjacent to the table with the computer.